The deltoid muscle consists of 3 fiber regions. The anterior portion flexes and medially rotates  the humerus. The posterior portion extends and laterally rotates the humerus. The middle portion abducts the humerus. From the rest position, the deltoid generates a superiorly directed vector that pulls the head of the humerus toward the acromion. The humeral head should not glide superiorly. If the posterior head of the deltoid has become the dominant lateral rotator, the result is anterior glide of the humeral head during motion. The humeral head should not glide anteriorly.
the humerus. The posterior portion extends and laterally rotates the humerus. The middle portion abducts the humerus. From the rest position, the deltoid generates a superiorly directed vector that pulls the head of the humerus toward the acromion. The humeral head should not glide superiorly. If the posterior head of the deltoid has become the dominant lateral rotator, the result is anterior glide of the humeral head during motion. The humeral head should not glide anteriorly.
If the anterior head if the deltoid has become a dominant medial rotator and/or the subscapularis, a medial rotator, is dominating the lateral rotators, the resting glenohumeral position is one of medial rotation. The combination of abduction and medial rotation predisposes the subject to an impingement syndrome.
It is essential that the depressors of the humeral head primarily the supraspinatus, infraspinatus, teres minor, and subscapularis adequately offset the proximal pull of the deltoid muscle. Continue reading
 the humeral head in the glenoid. Because this muscle passes under the acromion, it is particularly vulnerable to injury when the shoulder is depressed. If the humeral head glides superiorly, does not glide inferiorly during shoulder flexion and abduction, or does not rotate laterally enough to prevent impingement of the greater tuberosity against the coracoacromial ligament, then the supraspinatus muscle and tendon are exposed to compression forces.
the humeral head in the glenoid. Because this muscle passes under the acromion, it is particularly vulnerable to injury when the shoulder is depressed. If the humeral head glides superiorly, does not glide inferiorly during shoulder flexion and abduction, or does not rotate laterally enough to prevent impingement of the greater tuberosity against the coracoacromial ligament, then the supraspinatus muscle and tendon are exposed to compression forces.  this muscle limits shoulder flexion and can impede depression and lateral rotation of the humeral head.
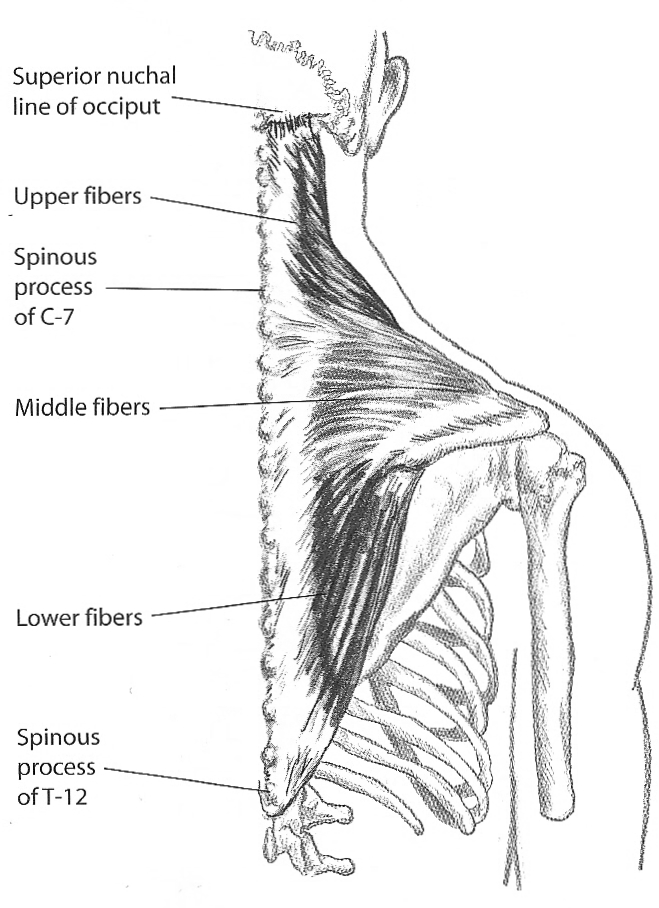
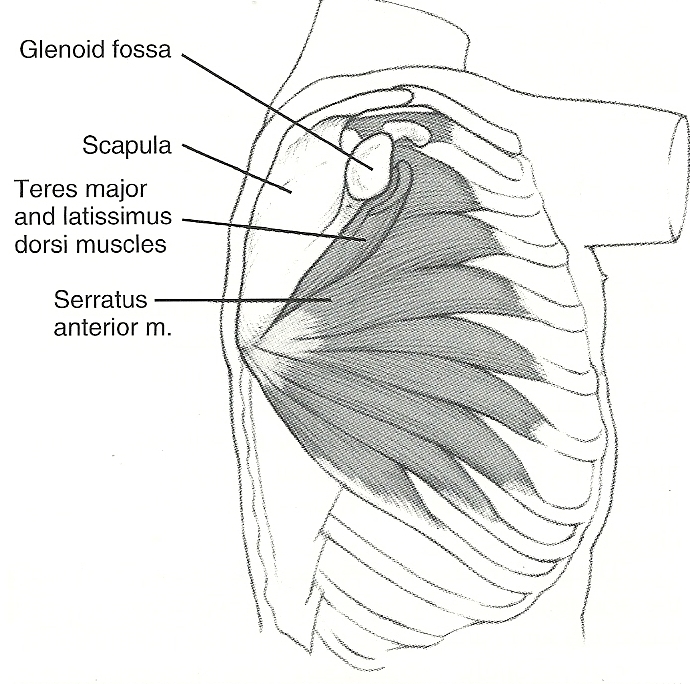
this muscle limits shoulder flexion and can impede depression and lateral rotation of the humeral head.  girdle (not the humeral head). The range of shoulder flexion/elevation is limited when the latissimus dorsi is short. When acting bilaterally, the latissimus dorsi extends the spine and anteriorly rotates the hips. If the abdominals are weak, shoulder flexion is compensated for with lumbar spine extension.
girdle (not the humeral head). The range of shoulder flexion/elevation is limited when the latissimus dorsi is short. When acting bilaterally, the latissimus dorsi extends the spine and anteriorly rotates the hips. If the abdominals are weak, shoulder flexion is compensated for with lumbar spine extension.  horizontally adduct the shoulder. The lower fibers depress the shoulder girdle through their attachments on the humerus. A common clinical finding is that the fibers forming the sternal portion of the pec major test short, while the fibers forming the clavicular portion test long.
horizontally adduct the shoulder. The lower fibers depress the shoulder girdle through their attachments on the humerus. A common clinical finding is that the fibers forming the sternal portion of the pec major test short, while the fibers forming the clavicular portion test long.