Excerpted from: (Page, Frank, Lardner. Assessment and Treatment of Muscle Imbalance, The Janda Approach. 2010, Human Kinetics, Champagne IL.)
Because of its versatility in positioning and posture, the shoulder may be predisposed to muscle imbalance syndromes, including shoulder impingement and rotator cuff tendinosis, thoracic outlet syndrome, and shoulder and neck pain.
The shoulder complex includes four articulations; the glenohumeral, scapulothoracic, acromioclavicular, and sternoclavicular joints. The synovial glenohumeral joint is supported by capsuloligamentous structures, but these actually provide little stability; instead, joint stabilization is provided by dynamic contraction of the rotator cuff during movement. The deltoid and biceps also stabilize the glenohumeral joint.
Contrary to anatomical description that the rotator cuff only performs humeral rotation, the primary role of the rotator cuff is stabilization and elevation in the scapular plane. Only mild contraction of the rotator cuff is necessary for stability, therefore rotator cuff strengthening programs do not necessarily have to fatigue the muscles to improve the function. In fact, fatigue of the rotator cuff can cause as much as 0.1 inch (2.5 mm) of unwanted upward migration of the humeral head during abduction. A decrease in in rotator cuff stabilizing force proportionally increases anterior displacement (anterior glide) of the humeral head.
While the rotator cuff plays plays the vital role in maintaining centration of the humeral head, it is the dynamic scapular stabilizers that coordinate the position of the glenoid with the humerus. Fatigue of the scapular stabilizers can significantly reduce rotator cuff strength. Scapular stabilization is critical for glenohumeral function since the rotator cuff originates on the scapula.
Scapulohumeral function is controlled by two main muscular force couples. These are the (1) rotator cuff and deltoid and (2) scapular rotators.
Rotator Cuff-Deltoid Force Couple
 The primary role of the rotator cuff is dynamic stabilization of the glenohumeral joint. Within the rotator cuff itself, a force couple between the subscapularis and the infraspinatus and teres minor provides a compressive force drawing the humeral head into the glenoid. This compressive force is described as parallel to the axiallary border of the scapula, or perpendicular to the glenoid. The net effect is a depressor force vector that counteracts the elevation force of the deltoid. This rotator cuff-deltoid force couple is key to shoulder abduction. In fact, the deltoid force needed for abduction is 41% less when the rotator cuff is activated along with deltoid contraction. The supraspinatus is more active at the beginning of ROM, while the deltoid is more active near the end.
The primary role of the rotator cuff is dynamic stabilization of the glenohumeral joint. Within the rotator cuff itself, a force couple between the subscapularis and the infraspinatus and teres minor provides a compressive force drawing the humeral head into the glenoid. This compressive force is described as parallel to the axiallary border of the scapula, or perpendicular to the glenoid. The net effect is a depressor force vector that counteracts the elevation force of the deltoid. This rotator cuff-deltoid force couple is key to shoulder abduction. In fact, the deltoid force needed for abduction is 41% less when the rotator cuff is activated along with deltoid contraction. The supraspinatus is more active at the beginning of ROM, while the deltoid is more active near the end.
Scapular Rotator Force Couple
The upper and lower trapezius are coupled with the serratus anterior to produce upward rotation of the scapula. Scapular rotation maintains the optimal length-tension relationship of the deltoid during abduction. The trapezius is more active during abduction than flexion and plateaus in EMG activity after 120˚.
Different parts of the trapezius have different histological characteristics that correspond to different functional demands. The lower trapezius is better suited for stabilization, while the upper trapezius is better suited for movement. The middle and lower trapezii maintain the vertical and horizontal position of the scapula rather than generate torque, working at a constant length to resist protraction of the scapula from the serratus anterior.
The lower trapezius relaxes during flexion and is not active until abduction. It becomes more active with shoulder elevation to assist the upper trapezius and serratus anterior in rotating the scapula upward. Proper balance between the upper trapezius and serratus anterior is believed to reduce the superior migration of the scapula, improve posterior scapular tilt, facilitate optimal glenohumeral congruency, and maximize the available subacromial space (SAS) under the coracromial arch to avoid impingement. If the lower trapezius is inhibited, the deltoid loses its length-tension relationship and may overwork the infraspinatus.
Muscle activation and timing are key not only to proper activation of the force couple but also to overall function of the shoulder complex. For example, if the mid- and lower trapezius react too slowly in relation to the upper trapezius, the upper trapezius may become overactive, leading to scapular elevation rather than upward rotation.
Often muscles are activated in a feed-forward mechanism. This preactivation stabilizes segments before movement initiation. For example, during rotation the rotator cuff and biceps are activated before the deltoid and pectoralis major, a finding that supports the suggested role of the rotator cuff and biceps in stabilizing the glenohumeral joint. In addition, the deltoid is activated before the trapezius, while the upper trapezius is activated before abduction.
Chain Reactions
The upper extremity forms a single kinetic chain from the upper spine to the fingers. The upper extremity is connected to the axial skeleton by only one true articulation: the sternoclavicular joint. For this reason, the shoulder complex relies on muscles to begin the kinetic chain to transfer forces from the trunk.
The proximal end of the kinetic chain begins in the cervical spine, thoracic spine, and ribs. The upper trapezius and levator scapula have origins in the cervical spine , while the middle trapezius and rhomboids originate in the thoracic spine. The ribs serve as an origin for the pectoralis major and serratus anterior. The upper thoracic spine extends, rotates, and laterally flexes during elevation in the sagittal and scapular planes. Thus, thoracic mobility is important in the upper-extremity kinetic chain.
There are several important muscle slings to consider in the upper extremity. Because 50% of the total force in overhand throwing comes from the legs and trunk the entire kinetic chain from the foot to the hand, particularly in athletes, should be considered during assessment of upper-extremity dysfunction.
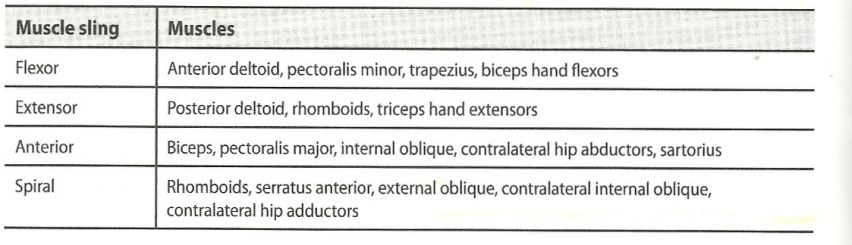
Muscle Slings of the Upper Extremity
The scapula provides the following:
- A stable glenohumeral articulation
- Protraction and retraction on the thoracic wall to position the arm
- Elevation of the acromiom to prevent impingement
- A base for muscle attachment (rotator cuff and scapular rotators)
- A link for transferring force proximally to distally in throwing
The importance of the kinetic chain is evident when describing pathomechanics of rotator cuff tendinitis. Poor scapular stabilization increases activity of the upper trapezius for stabilization, which in turn increases scapular elevation. Scapular elevation alters the direction of the axis of the glenoid fossa. This change may be accompanied by increase and constant activity in the rotator cuff, leading to rotator cuff tendinitis.
Motor patterns in both the upper and lower extremities are influenced by the upper extremity. When a person is standing, elevation of the shoulder activates the contralateral erector spinae as well as the lower extremity muscles to maintain postural stability. This activation results from feed-forward motor control used to stabilize the trunk before arm movement begins, regardless of the direction of the arm movement.
Again, pathology demonstrates the influence of the kinetic chain; patients with shoulder and neck pain demonstrate poor postural stability. This phenonmenon indicates a disruption in the feed forward mechanism (see ), indicating CNS involvement in mediating chronic shoulder pain.
