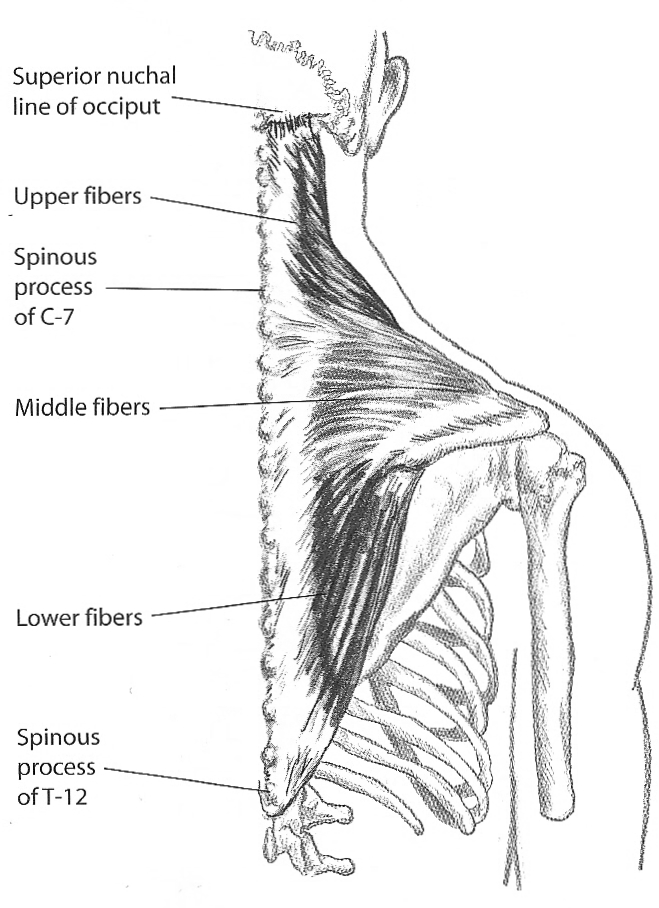
- The trapezius muscle adducts and upwardly (laterally) rotates the scapula.

- The upper fibers are more suited for movement, and elevate the scapula.
- The middle and lower fibers maintain the vertical and horizontal position of the scapula rather than generate torque. They are better suited for stabilization, working at a constant length to resist protraction of the scapula by the serratus anterior.
- Some authors suggest that the middle fibers adduct the scapula, while the lower fibers depress the scapula. Thus, when the upper trap is short and the lower fibers are overstretched and weak the entire shoulder girdle will be elevated, rather than upwardly rotated.
- When he upper trapezius is short, and the shoulder girdle is posturally elevated, the entire shoulder, including the distal end of the acromiom, should be elevated.
- If the upper trap is overstretched and weak and the lower fibers are short and facilitated, the shoulder may be depressed.
- If the scapula fails to elevate during shoulder flexion or abduction, the action of the upper trapezius is considered to be insufficient.
- If the middle fibers are short and tight, adduction may dominate over abduction.
Category Archives: Thoracoscapular Muscles
Serratus Anterior
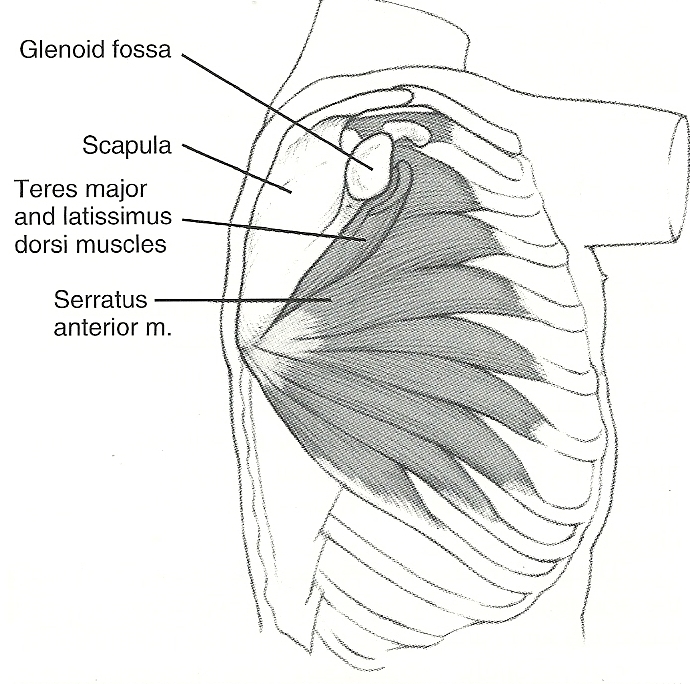
- The serratus anterior muscle abducts and upwardly (laterally) rotates the scapula and holds the scapula flat against the rib cage. The upward rotation is produced by the force couple action of the serratus anterior muscle and the trapezius muscle.
- The serratus anterior is the primary, and only effective abductor of the scapula.
- Full range of flexion/elevation motion is not possible if the serratus anterior is paralyzed or weak.
- Impaired control of the scapula by the serratus anterior is common, and results from the serratus being weak, long, short, or altered in the timing of its movement of the scapula. If the scapula is not correctly positioned during shoulder flexion or abduction the scapulohumeral muscles (rotator cuff) will not be able to maintain their optimal length and tension relationships.
- Deficient control of the serratus anterior, causing impairment in timing and range of scapular motion, can cause stress at the glenohumeral joint. This stress results from the incorrect positioning of the glenoid for glenohumeral joint motion when there is insufficient abduction and upward rotation of the scapula.
 Observation of the degree of abduction or adduction of the scapula is necessary to distinguish insufficient performance of the trapezius or serratus anterior.
Observation of the degree of abduction or adduction of the scapula is necessary to distinguish insufficient performance of the trapezius or serratus anterior.- Although both muscles are upward rotators, because the trapezius is an adductor and the serratus an abductor, the medial/lateral position of the scapula can be a guide as to which muscle should be emphasized for lengthening or strengthening.
- The primary indicators of impaired performance are inadequate abduction and inadequate upward rotation of the scapula during shoulder flexion and abduction.
Rhomboids

Posterior Right
The rhomboid muscles adduct and downwardly and (medially) rotate the scapula. The rhomboids, like the levator scapula, are both synergists and antagonists of the trapezius. The rhomboids typically become more dominant than the trapezius and will restrict upward rotation of the scapula. Depressed shoulders are a common postural impairment, which leaves the upper trapezius frequently overstretched and weak.
Shoulder shrugging exercises with the arms down only reinforces the dominance of the rhomboids and levator scapula. To emphasize upper trapezius activity shoulder shrugging should be done with the arms overhead so that the scapula is upwardly rotated. Continue reading
Pectoralis Minor
The pectoralis minor muscle tilts the scapula forward (anteriorly) by pulling the coracoid process forward and downward (caudally). Shortness of this muscle interferes with upward rotation of the scapula and can restrict elevation of the rib cage. If the abdominals are short and stiff, this restriction is even more exaggerated, adding greater resistance to movement of the scapula.
process forward and downward (caudally). Shortness of this muscle interferes with upward rotation of the scapula and can restrict elevation of the rib cage. If the abdominals are short and stiff, this restriction is even more exaggerated, adding greater resistance to movement of the scapula.
Shortness of the pec minor can also contribute to thoracic outlet syndrome (TOS).
This muscle is difficult to stretch because pressure must be applied at the coricoid process, not the humerus.
When correcting the scapular position, the glenohumeral joint must remain in neutral position. the emphasis must be on posterior tilt and not adduction of the scapula.
Levator Scapula

Right Posterior View
The levator scapula muscle adducts and downwardly (medially) rotates the scapula and is a synergist of the trapezius for adduction but an antagonist for rotation.
The levator scapula (LS) attaches to the transverse processes of the first 4 cervical vertebrae, and can restrict cervical rotation, but in the presence of excessive cervical joint flexibility may rotate the cervical spine during shoulder motions.
During shoulder flexion, the LS is stretched as the scapula upwardly rotates. If the LS is ‘stiff’ (limited extensibility) the stretch of the muscle can rotate the head to the ipsilateral (same) side.
Because this muscle attaches to the medial aspect of the superior angle of the scapula. Shortness of this muscle can limit upward rotation of the scapula and can give the impression of an elevated shoulder when observing the shoulder height near the base of the neck.
The attachment of the LS to the superior angle of the scapula can elevate the most medial portion of the scapula but does not elevate the acromial region. During shoulder flexion, the LS is stretched as the scapula upwardly rotates. The LS can elevate the most medial portion of the scapula, but does not elevate the acromial region. It is also important to differentiate between shortness of the levator scapula and rhomboids versus the upper trapezius in the treatment phase. Continue reading
