Indications
Toning weakened musculature. Continue reading
Indications
Toning weakened musculature. Continue reading
Indications
Indications
Indications
Indications
This technique involves using the position of ease as part of a sequence which commences with the location of a tender/pain/trigger point, followed by the application of ischemic compression (this is optional and is avoided if the pain is too intense or the patient too fragile or sensitive) followed by the introduction of positional release as described by McPartland and Zigler (1993)… ‘Any painful point as a starting place for SCS’.
After an appropriate length of time during which the tissue are held in a position of ‘ease’, the patient is asked to introduce an isometric contraction into the affected tissues for 7-10 seconds, after which these are stretched (or they may be stretched at the same time as the contraction, if fibrotic tissue calls for such attention).
Note: the introduction of muscle energy technique (MET).
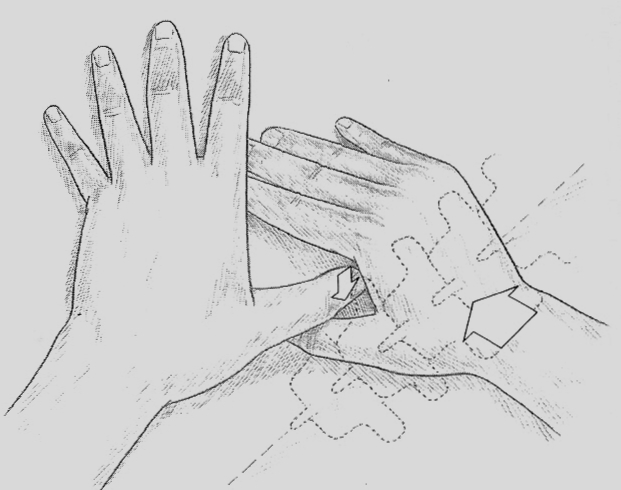
Marsh Morrison suggested very light palpation, using extremely light touch, as a means of feeling a ‘drag’ sensation alongside the spine (as lateral as the tips of the transverse processes). Drag relates to increased hydrosis, which is a physiological response to increased sympathetic activity and is an invariable factor in skin overlying trigger and other forms of reflexively induced or active myofascial areas. Once drag is noted, pressure into the tissues normally evinces a report of pain.
The operator stands on the side of the prone patient opposite the sid in which pain has been discovered in these paraspinal tissues.
Once located, tender or painful points (lying no more lateral than the tips of the transverse processes) are palpated for their sensitivity to pressure. Once confirmed as painful, the point is held by firm thumb pressure while, with the soft thenar eminence of the other hand, the tip of the spinal process most adjacent to the pain point is very gently eased towards the pain (ounces of pressure only), so crowding and slackening the tissues being palpated, until pain reduces by at least 75%. Direct pressure of this sort (lightly applied) towards the pain should lessen the degree of tissue contraction and the sensitivity.
If it does not do so, then the angle of the push on the spinous process towards the painful spot should be varied slightly so that, somewhere within an arc embracing a half circle, an angle of push towards the pain will be found to abolish the pain totally and will lessen the feeling of tension. This position is held for 20 seconds after which the next point is treated. A full spinal treatment is possible using this extremely gentle approach which incorporates the same principles as SCS and functional technique, the achievement of ease and pain reduction as the treatment focus.
This variation on the theme of functional and SCS methods involves the positioning of the distressed area into the direction of its greatest freedom of movement, starting from a position of neutral in terms of the overall body position.
To start, the patient’s posture is modified to take the body, or part (neck for example) into a more ‘neutral’ position; maybe some balance between flexion and extension (whatever is appropriate). This is followed by an application of facilitating force (usually a crowding of the tissues). No pain monitor is used but rather a palpating/listening hand is applied (as in functional technique) which senses for changes in ease and bind in distressed tissues as the body/part is carefully positioned and repositioned. The final ‘crowding of the tissues’, to encourage a ‘slackening’ of local tension, is the facilitated aspect of the process, according to its theorists.
This ‘crowding’ might involve compression applied through the long axis of a limb perhaps, or directly downwards through the spine via cranially applied pressure, or some such variation.
The length of time the position of ease is held is usually suggested at just 5 seconds. It is claimed that altered tissue texture, either surface or deep, can be successfully treated in this way.
All areas which palpate as tender are responding to, or are associated with, some degree of imbalance, dysfunction, or reflexive activity which may well involve acute or chronic strain. Unlike Jones’ approach which begins from the viewpoint of identifying the likely position of tender points relating to particular strain positions, it makes just as much sense to work the other way around and to identify where the strain is likely to have occurred in relation to any pain point which has been identified. We might therefore consider that any painful point found during soft tissue evaluation or palpation, including a search for trigger points, could be treated by positional release, whether we know what strain produced them or not, and whether the problem is acute or chronic.
Experience and logic tell us that the response to positional release o0f a chronically fibrosed area will be less dramatic than from tissues held in simple spasm or hypertonicity. Nevertheless, even in chronic settings, a degree of release and ease can be produced, allowing for easier access to the deeper fibrosis.
This approach, of being able to treat any painful tissue using positional release, is valid whether the pain is being monitored via feedback from the patient, or by palpation alone.
As previously described, a period of 60-90 seconds is recommended as the time for holding the position of maximum ease.
Orthopedic functional technique ignores tenderness as its guide to the position of ease and relies instead on reduction in palpated tone in stressed (hypertonic/spasm) tissues as the body (or part) is being positioned or fine-tuned in relation to all available directions of movement in a given region.
A position of combined ease is achieved using what is known as a ‘stacking’ sequence. One hand palpates the affected tissues (molded to them without invasive pressure). This is described as the ‘listening’ hand since it assesses changes in the tone as the operator’s other hand guides the patient (or part) through a sequence of positions which are aimed at enhancing ease and reducing bind.
A sequence of evaluations is carried out, each involving different directions of movement (flexion, extension, rotation, side-bending, translation, distraction etc.) with each starting at the point of maximum ease discovered during the previous evaluation, or combined point of ease of a number of previous evaluations. In this way, one position of ease is ‘stacked’ on to another until all directions of movement have been assessed for ease. A position of maximum ease will be arrived at which is held (for the appropriate time) until there is a palpable release producing a reduction in pain.
The precise sequence in which the various directions of motion are evaluated is irrelevant, as long as all possibilities are included.
Theoretically (and usually, in practice) the position of maximum ease (reduced tone) in the distressed tissues should correspond with the position which would have been found were pain being used as the guide as in the previously described approaches.
