Cervical Spine Muscle Energy Technique
Typical Cervical Vertebra (C5-C6)
Diagnosis
Position: Flexed, rotated left, and side-bent left (FRSleft)
Motion Restriction: Extension, right rotation, and right side-bending (ERSright)
The C5 right facet won’t close.
Treatment
Patient is supine on the table with the operator sitting at the head of the table.
Operator’s finger tips of the right index and middle finger are placed on the right articular pillar of C6 to hold the segment so that C5 can be moved upon it.
Operator’s left hand controls the left side of the patient’s head and neck.
Operator’s right fingers translate the segment anteriorly introducing motion to the backward-bending barrier.
Operator’s left hand introduces right side-bending and rotation of the head and neck to the right by right to left translation engaging the right rotation and the right side-bending barriers.
Patient exerts a small isometric effort against the operator’s resisting left hand into forward bending, left side-bending, or left rotation.
After a 3-5 second muscular effort, the patient relaxes and the operator increases translatory movement in an anterior and right to left direction engaging the backward-bending, right side-bending, and right rotation barriers. This process is repeated 3-5 times.
Retest.





 monitoring the first movement of the atlas.
monitoring the first movement of the atlas.



 through the external auditory meatus while monitoring for the first movement of the atlas.
through the external auditory meatus while monitoring for the first movement of the atlas. to forward bending, right side-bending, and left rotation (ESleftRright). Something interfered with the left condyle’s ability to glide posteriorly.
to forward bending, right side-bending, and left rotation (ESleftRright). Something interfered with the left condyle’s ability to glide posteriorly. motion restriction is to forward bending, left side-bending, and right rotation (ESrightRleft). Something interfered with the right condyle’s ability to glide posteriorly.
motion restriction is to forward bending, left side-bending, and right rotation (ESrightRleft). Something interfered with the right condyle’s ability to glide posteriorly.
 resistance to movement at his index fingers. If resistance is felt, motion restriction is to backward bending, right side-bending, and left rotation (C0 flexed [F], side-bent left [Sleft], and rotated [Rright]. Something interfered with the right condyle gliding forward.
resistance to movement at his index fingers. If resistance is felt, motion restriction is to backward bending, right side-bending, and left rotation (C0 flexed [F], side-bent left [Sleft], and rotated [Rright]. Something interfered with the right condyle gliding forward. encountered, the restriction is to backward bending, left side-bending, and right rotation (FSrightRleft). Something interfered with the left condyle gliding forward.
encountered, the restriction is to backward bending, left side-bending, and right rotation (FSrightRleft). Something interfered with the left condyle gliding forward. restriction of the typical cervical segment rotation through ligamentous locking. Neck flexion must be maintained throughout the procedure.
restriction of the typical cervical segment rotation through ligamentous locking. Neck flexion must be maintained throughout the procedure. rotated left).
rotated left). rotated right).
rotated right).
 his index fingers. If resistance is felt, the motion restriction is to forward-bending, right side-bending, and right rotation (indicating that the segment is extended, rotated and side-bent left [ERSleft]). Something has interfered with the capacity of the left facet to open.
his index fingers. If resistance is felt, the motion restriction is to forward-bending, right side-bending, and right rotation (indicating that the segment is extended, rotated and side-bent left [ERSleft]). Something has interfered with the capacity of the left facet to open. his index fingers. If resistance is felt, the motion restriction is to forward-bending, left side-bending, and left rotation (indicating that the segment is extended, rotated, and side-bent right [ERSright]). Something has interfered with the capacity of the right facet to open.
his index fingers. If resistance is felt, the motion restriction is to forward-bending, left side-bending, and left rotation (indicating that the segment is extended, rotated, and side-bent right [ERSright]). Something has interfered with the capacity of the right facet to open.


 operator introduces translation from right to left, sensing for resistance to movement at his index fingers. If resistance is felt, the motion restriction is to backward-bending, right side-bending, and right rotation (indicating that the segment is flexed, rotated and side-bent left [FRSleft]). Something has interfered with the capacity of the left facet to close.
operator introduces translation from right to left, sensing for resistance to movement at his index fingers. If resistance is felt, the motion restriction is to backward-bending, right side-bending, and right rotation (indicating that the segment is flexed, rotated and side-bent left [FRSleft]). Something has interfered with the capacity of the left facet to close. operator introduces translation from left to right, sensing for resistance to movement at his index fingers. If resistance is felt, the motion restriction is to backward-bending, left side-bending, and left rotation (indicating that the segment is flexed, rotated, and side-bent right [FRSright]). Something has interfered with the capacity of the right facet to close.
operator introduces translation from left to right, sensing for resistance to movement at his index fingers. If resistance is felt, the motion restriction is to backward-bending, left side-bending, and left rotation (indicating that the segment is flexed, rotated, and side-bent right [FRSright]). Something has interfered with the capacity of the right facet to close.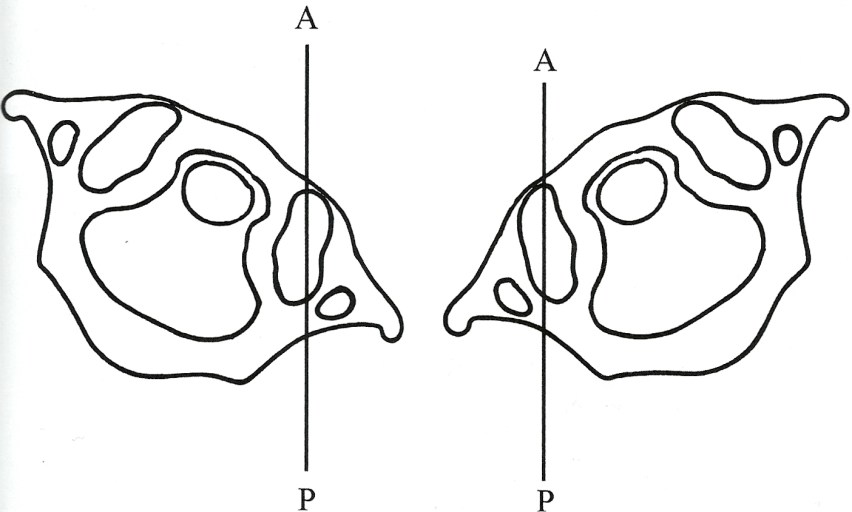
 rotation of the head sensing for prominent fullness under the right thumb indicating posterior rotation of the atlas on the left.
rotation of the head sensing for prominent fullness under the right thumb indicating posterior rotation of the atlas on the left. and left rotation of the head and monitors for prominence of the right posterior arch of the atlas under the right index finger, indicative of right rotation of the atlas.
and left rotation of the head and monitors for prominence of the right posterior arch of the atlas under the right index finger, indicative of right rotation of the atlas. rotation with the left hand while monitoring for prominence of the right posterior arch of the atlas under the right index finger, indicating atlas right rotation.
rotation with the left hand while monitoring for prominence of the right posterior arch of the atlas under the right index finger, indicating atlas right rotation. rotation of the head with the left hand while monitoring for prominence of the left posterior arch of the atlas under the right thumb, indicating left rotation of the atlas.
rotation of the head with the left hand while monitoring for prominence of the left posterior arch of the atlas under the right thumb, indicating left rotation of the atlas.


