Author Archives: John Castle
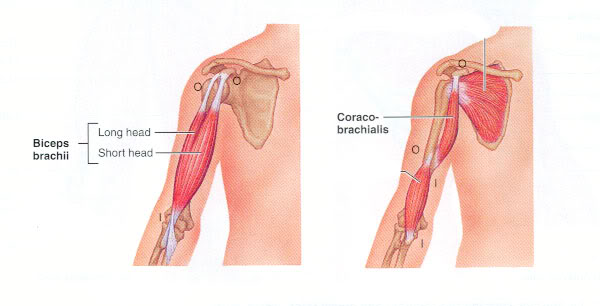
Subscapularis Tendinosis versus Bicipital and Coracobrachialis Tendinosis
These conditions are typically called tendinitis. A better term for both of these conditions might be tendon pain or tendinosis, which is the tearing of tendon fibers, due to repeated stress or overload, in the absence of an inflammatory process. It is important to perform muscle resistance testing to determine which of these muscles are causing anterior shoulder pain.
The long head of the biceps tendon and the subscapularis tendon lie next to each other and general palpation may not be able to determine which muscle is creating the tendon pain. Even though the pain may be in the same area, the treatment protocol and subsequent stretching are drastically different.
Subscapularis Treatment: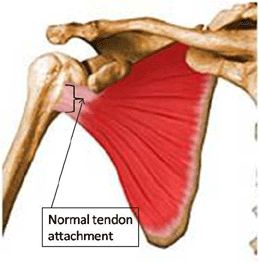
- Follow the shoulder protocol starting with the velvet glove technique.
- You will need to release all the other anterior shoulder muscles—pectoralis major, minor, and subclavius—before you work this muscle.
- Next, follow the specific protocol for the subscapularis including multi-directional friction and eccentric contraction.
- This is an extremely rare injury, as this muscle has a broad, flat, wide tendon, that is very deep and well protected. Although this muscle is almost always tight, subscapularis tendinosis is rare.
Biceps and Coracobrachialis Treatment:
- Start with the basic shoulder protocol and release all of the anterior shoulder muscles.
- The client is supine with the arm supinated, with support under the elbow using a bolster or a towel. Have the client perform a resisted test with the shoulder flexed to 90˚, palm facing up, to pinpoint the injury.
- Follow the rest of the specific biceps/coracobrachialis protocol.
- Continue to reassess and repeat any or all of the protocol until the client is pain-free.
Sitting Dx: Typical Vertebrae (C3-C7)
Patient sits on table or treatment stool.
Operator stands behind with the thumb and index finger contacting zygopophysial joints bilaterally with the left hand on the vertex of the head to control motion.
Operator’s left hand introduces forward-bending, right side-bending, and right rotation while monitoring left zygopophysial joint for opening movement.
Operator introduces forward-bending, left side-bending, and left rotation, palpating for opening of the right zygopophysial joint by the operator’s right index finger
Operator’s left hand introduces backward-bending, right side-bending, and right rotation with the right index finger monitoring the right zygopophysial joint’s capacity to close.
Operator introduces backward-bending, left side-bending, and left rotation with the left hand while monitoring the left zygopophysial joint’s capacity to close with the right  thumb.
thumb.
Structural Diagnosis
The anatomy and biomechanics of the cervical spine result in five somatic dysfunctions. The typical cervical segments (C3-C7) have non-neutral dysfunction with either a forward-bending or backward-bending restriction together with a coupled side-bending and rotation restriction to the same side (Type II motion).
At the atlantoaxial (C1-C2) junction, the primary somatic dysfunction is that of restriction of rotation to one side or the other. While there may be minor forward/backward-bending and side-bending components to the rotational restriction, adequate treatment to the rotational restriction restores the minor movement motion simultaneously.
At the occipitoatlantal (C0-C1) junction, there are two dysfunctions possible. There will either be forward-bending or backward-bending restriction with coupled side-bending and rotation to opposite side (Type I motion).
The structural diagnostic process starts by identifying levels of palpable deep muscle hypertonicity. This identifies segments that need motion testing. The diagnostic and the therapeutic processes seem to be most satisfactory by beginning from below and moving cephalad.
The bony landmark of most value in the typical cervical segment is the articular pillar. They are palpated in the deep fascial groove between the semispinalis medially and the cervical longissimus laterally. The paired examiner’s fingers can localize to the right and left articular pillars of any given cervical segment and introduce motion testing.
The typical cervical segment pillar is the size of the examiner’s finger pad. The identification of the articular pillars begins by first identifying the spinous process of C2 and C7. The C2 spinous process is the first bony prominence in the midline caudad to the external occipital protuberance (inion). The spinous process of C7 (vertebra prominens) is the spinous process that remains palpable during cervical backward-bending. The articular pillars of C2 and C7 are at the same level as the spinous processes. Placing the examiner’s fingers between the pillars of C2 and C7 puts the finger pads in contact with with C3, C4, C5, and C6. This provides the ability to localize to any specific cervical segment. The structural diagnostic process can be performed in patients in both sitting and supine positions.
Ideal Alignment of the Cervical Region
Ideal alignment of the cervical region allows the head to be positioned with minimal muscular effort. Ideal alignment is an inward lordotic curve with both the upper and lower cervical region in a position of slight extension.
The most common alignment impairment observed in the cervical spine is a forward head posture. The forward head posture is characterized by a forward translation of the lower cervical region, and hyperextension of the cervical region with typicaly, an increased kyphotic curve in the thoracic region.
Normal Forward Head




The muscular adaptations associated with a forward head position are shortening of the cervical spine extensors and a lengthening of the intrinsic cervical spine flexors. The forward head position also requires increased activity of the extensor muscles of the cervical spine to counter balance the head against the effect of gravity. The muscular adaptations that occur with a forward head position results in an increase in compressive forces acting on the articular facets.
Additional alignment faults may include an increase in the degree of upper cervical extension in comparison to that of the lower cervical spine, suggesting possible muscular adaptations in the suboccipital region. These adaptations can include shortness of the suboccipital extensors, superior obliques, inferior obliques, and rectus capitus and lengthened position of the suboccipital flexors, rectus capitus lateralis and anterior muscles.
Motions of the Cervical Spine
The cervical spine consists of seven vertebrae that are divided into two distinct regions. The upper region consists of the occiput, C1, and C2 vertebrae and lower region includes the vertebrae of C3-C7. Precise movements of the cervical spine require optimal arthrokinematics and osteokinematics and depend on muscle length, strength, and recruitment patterns. Motions of the cervical spine are comprised of coupled motions.
Neutral mechanics, also known as Type1 mechanics, result in coupled movement of side bending and rotation to opposite sides. Neutral mechanics occur in the thoracic and lumbar spine. Non-neutral mechanical coupling, or Type2 mechanics occur when side bending and rotation of vertebrae occur to the same side.
C0 = occiput, C1 = atlas, C2 = axis, C3-C7 = typical
Atlas
The primary movement of the occipitoatlantal articulation (C0-C1) is forward and backward bending. There is also a small amount of coupled side bending and rotation to opposite sides. Left rotation of the occiput on the atlas is associated with anterior displacement of the right occipital condyle on the right articular process of the atlas. As the occiput turns to the left, the occipital condyles are displaced to the left, resulting in side bending to the right.
Axis
The geometry and orientation of the C0-C1 and C1-C2 articular processes appear to dictate the type and amount of motion available at the atlantoaxial joint. The primary movement here is rotation. (There is no intervertebral disc between C1 and C2.)
Typical Cervical Vertebrae
Intervertebral discs are found between two typical vertebral bodies. At the posterolateral corner of each vertebral body is a small synovial joint called the uncovertebral joint of Luschka. These joints are found only in the cervical region and are subject to degenerative changes that occasionally encroach on the intervertebral canal posteriorly. Flexion, extension, side bending, and rotation are all permissible in the typical cervical vertebrae; lateral flexion and rotation are always facet controlled. Side bending in one direction will always be coupled with rotation in the opposite direction (Type 1 mechanics).
Muscle Actions of the Cervical Spine
Optimal muscle lengths and recruitment patterns are critical to the performance of cervical motions to allow the ideal ratio of coupled motion to occur. The muscles of the cervical region can be classified into two distinct groups according to the relationship of the attachment of the muscle to the axis of motion of the cervical spine. The intrinsic muscles of the cervical spine located close to the axis of motion are felt to control precise control of motion during movement. The extrinsic muscles of the cervical spine are located farther from the axis of motion and provide power to the motion but not necessarily precision of motion. A balance of participation between these two groups is critical for precise and pain-free motion of the cervical spine.
Cervical Flexors
 The function of the intrinsic cervical flexors is to produce forward sagittal plan rotation or ‘rolling’ of the cervical vertebrae. The muscles producing the sagittal rotation motion in the upper cervical region are the rectus capitis anterior and rectus capitis lateralis.
The function of the intrinsic cervical flexors is to produce forward sagittal plan rotation or ‘rolling’ of the cervical vertebrae. The muscles producing the sagittal rotation motion in the upper cervical region are the rectus capitis anterior and rectus capitis lateralis.
In the lower cervical region, forward sagittal rotation is produced by the longus capitis and longus coli. The longus capitis and longus coli are also active in protecting the anterior structures during forceful extension motions.
The function of the extrinsic cervical flexors is to add force to the flexion movement and produce flexion motion associated with forward translation of the cervical vertebrae. The muscles contributing to the forward translator motion in the cervical region are the sternocleidomastoids and the anterior and medial scalenes. Commonly, these muscles are dominant during flexion movements. The dominant effect of the extrinsic muscles can result in a faulty movement pattern of anterior translation of the head and cervical spine with diminished anterior sagittal plane rotation.


Cervical Extensors
The function of the intrinsic cervical extensors is to produce sagittal rotation or backward ‘rolling’ of the cervical vertebrae. The muscles attributed to producing the posterior sagittal rotation in the upper cervical region are the rectus capitis posterior major and minor, the oblique capitis inferior and superior, and the semispinalis capitis,the spelnius capitis, and the longissimus capitis.


The muscles in the lower cervical region that produce posterior sagittal rotation are the semispinalis cervicis, the splenius cervicis, and the longissimus cervicis.


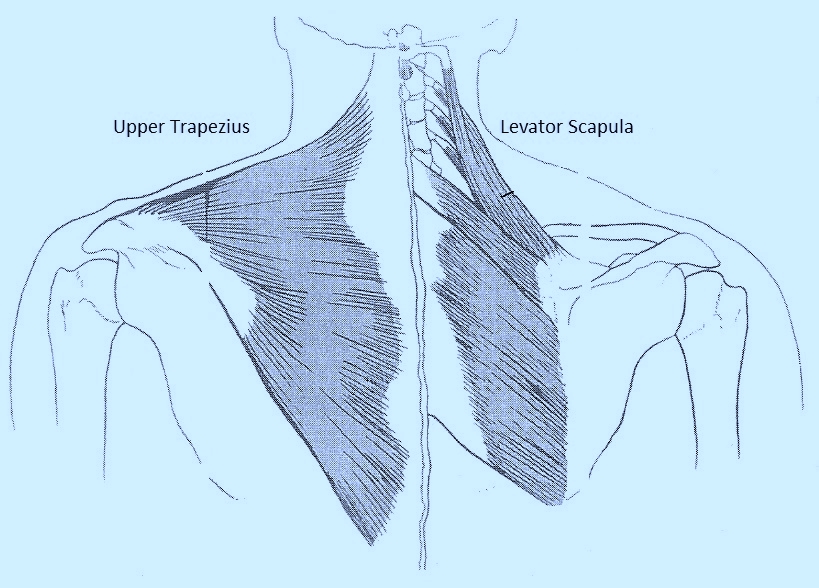
The function of the extrinsic cervical extensors is to produce extension with posterior translation of the cervical vertebrae. The muscles attributed to producing this posterior translator motion in the cervical region are the upper trapezius and levator scapulae. A common faulty recruitment pattern can include greater recruitment of the extrinsic cervical extensors during cervical extension, and can be best observed in the prone or quadruped position.
Cervical Rotators
The intrinsic cervical rotators produce rotation about a vertical axis. These muscles include the rectus capitis posterior major, the oblique capitis inferior, the oblique capitis superior, and the splenius.
The extrinsic cervical rotators include the sternocleidomastoids, the scalenes, the upper trapezii, and the levator scapulae. These muscles all have the action of rotation but also the simultaneous action of lateral flexion. If these muscle groups are dominant during rotation, the precision of movement about a vertical axis may be compromised.
The therapist will often observe rotation with concurrent lateral flexion, complaining of pain when the lateral flexion occurs, and pain-free ROM when concurrent lateral flexion is avoided.
The therapist may also observe rotation with simultaneous extension. This faulty movement pattern may be an indication of dominance of the sternocleidomastoid and its influence as an extensor of the upper cervical spine over the poorly recruited intrinsic cervical rotators which would maintain motion about a vertical axis. The actions of the upper trapezius and levator scapulae can also contribute to cervical extension during rotation.
In addition, the therapist may observe cervical rotation with simultaneous flexion and/or forward translation of the head and neck. This faulty movement pattern may be an indication of dominance of the anterior scalenes, the middle scalenes, and the sternocleidomastoids during the movement of rotation.
Manually guiding the patient’s pattern of rotation is often necessary. A frequent intervention is to instruct the patient to turn the head and neck easily to reduce the magnitude of muscular contractions and encourage a more appropriate muscle recruitment pattern. Strong muscle contractions, especially of the extrinsic rotators can add compression to the cervical spine structures.
In addition, the ‘extrinsic’ upper trapezius and levator scapulae are attached from the cervical spine region directly to the scapula and clavicle. The clinical significance is that single arm movements can result in compensatory motion of rotation of a cervical spine segment or several segments. Even the passive stretch of the trapezius and levator scapula (arms hanging at your side) will influence the ROM during active cervical motions, especially rotation, which can result in pain.
Protected: Waslaski’s Cervical Spine
The Cervical Spine
 The cervical spine is an important region of the vertebral column in the field of manual medicine. It receives a great deal of attention by manual medicine practitioners. It functions as the support of the skull and biomechanically provides mobility for a number of activities of daily living. A myriad of head, neck, and upper extremity symptoms have been observed when the cervical spine is dysfunctional. Symptomatic conditions in the area can be categorized as cervicocephalic syndrome, cervical syndrome, and cervicobrachial syndrome.
The cervical spine is an important region of the vertebral column in the field of manual medicine. It receives a great deal of attention by manual medicine practitioners. It functions as the support of the skull and biomechanically provides mobility for a number of activities of daily living. A myriad of head, neck, and upper extremity symptoms have been observed when the cervical spine is dysfunctional. Symptomatic conditions in the area can be categorized as cervicocephalic syndrome, cervical syndrome, and cervicobrachial syndrome.
The cervicocephalic syndrome includes pain and restriction of motion of the upper cervical spine and associated superficial and deep pain in the head. This syndrome often demonstrates alteration in vision, vertigo, dizziness, and nystagmus.
The cervical syndrome includes painful stiffness of the neck of varying severity from mild to acute spastic torticollis.
The cervicobrachial syndrome couples painful stiffness of the cervical spine with symptoms in the shoulder girdle and upper extremity. The upper extremity symptoms result from alteration of the functional capacity of the brachial plexus or altered vascular function through the arterial, venous, and lymphatic systems. Associated dysfunctions of the thoracic inlet, particularly the first and second ribs and in the thoracic spine and rib cage as far as T5 or T6, contribute to the cervicobrachial syndrome.
The cervical spine is subjected to acute injuries such as the flexion-extension “whiplash” injury and chronic repetitive injury from improper posture and abnormal positions of the head and neck. It is common in our culture to patients with forward head carriage as a component of poor posture.
Forward head posture results in an increase in the upper cervical lordosis and a flattening of the lower cervical spine. The balance of the head on the neck is altered, resulting in muscle imbalance with resulting tightness of the neck extensors and weakness of the deep neck flexors.
The clinical practitioner must understand the anatomy, physiology, and biomechanics of the region to understand the therapeutic role of manual therapy and avoid potential complications.
The cervical spine is particularly susceptible to degenerative forces arising from repeated movements, prolonged postures, and simply through the process of aging. The cervical spine is particularly susceptible to degenerative changes because normal day-to-day activities require frequent movement of the head and cervical spine. The inevitable degeneration process leads to injury, altering the precision of movement that negatively impacts the rate and type of degeneration.
The onset of painful and degenerative conditions of the cervical spine is precipitated by deviations in alignment and movement patterns. The clinical practitioner must be particularly familiar with the normal anatomy and kinesiology of the cervical spine to form the basis for understanding and recognizing abnormal motion.
Optimal alignment and movement patterns are believed to slow the degenerative process. Therefore, good posture and optimal movement patterns should be understood and practiced.
Neck and shoulder pain
Jen presented on a Physician referral for ‘neck pain’ that had persisted for more than 12 months. This pain was limited to neck, upper trapezius, and levator scapula regions. She was not experiencing any numbness, pain or other symptoms down her arms, or in her hands. She is a teacher who works with special needs children who are at a pre-school age. Her job requires her to squat and/or bend down and lift children constantly. She’d already had an MRI. Her physician felt that the neck pain might be being caused by some disc degeneration, and/or slightly bulging discs. Previous physical therapy appointments over the course of her symptoms had been ineffective. Her physician referred her to me, as somewhat of a last resort.
A postural assessment strongly suggested the presence of both upper and lower-cross syndrome (layer syndrome). Her upper posture included forward head, increased cervical lordosis, rounded shoulders, and increased thoracic kyphosis. Her whole primary anterior curve appeared short, suggesting a short superficial front line, which would include short/weak rectus abdominus and probably short/tight hip flexors. Her lower posture was characterized by hyper-lordotic lower back and anteriorly rotated pelvis, which also suggested a short/tight hip flexor complex, tight lumbar region, weak abdominals and weak gluteus maximus.
Initially, the transverse alar ligament test, vertebral artery compression test, and cervical compression/decompression were performed as contraindicative ‘precautionary’ tests. These precautionary tests were all negative, and were followed by active range of motion testing of the cervical spine which included cervical flexion, extension, left and right lateral flexion, and left and right rotation. AROM for flexion (80˚) and extension (65-70˚) were both WNL but guarded due to discomfort. Lateral flexion was guarded on both sides with some restriction L (15-20˚) and R (20-25˚). Lateral flexion elicited pain in the levator scapula and cervical region on both sides. Rotation was the most guarded and restricted with L (65˚) and R(60˚).
Following this assessment (during her first visit) I gently proceeded through the first part of the cervical protocol which included Dural Mater and Dural Sheath Mobilization, Atlanto-Occipital/Atlanto-Axial Lateral Mobilization, Atlanto-Occipital/Atlanto-Axial Anterior-Posterior Mobilization, Velvet Glove Myofascial Release Technique, SCM/Scalene Protocol, Cervical Spine Mobilization Techniques, and the interspinales/rotatores/intertransversarii release. All these techniques helped to significantly reduce her discomfort and improve her restricted ranges of motion. To say the least, Jen was both surprised at the results and grateful for the pain relief, which was significant.
Two days later Jen returned for her second session. Her neck pain was reduced by 80%. She couldn’t believe it. The session I had planned for that day started with some elements of the shoulder protocol to begin addressing the upper-cross issues. I was particularly focused on releasing the pec, pec minor, sub-scap, middle deltoid, and upper trapezius before I began the cervical work. This time around, I completed the entire cervical protocol starting at the beginning but adding the suboccipitals and levator scapula releases, upper thoracic work and neck decompression, and stretching during therapy. At the end of the session, I went over the home stretching exercises and explained their importance. I included both cervical and shoulder stretches. Then I instructed her on the appropriate strengthening exercises, and made copies from the self-care manual of all appropriate stretching and strengthening exercises for her to take home. Again, the outcomes at the end of the session were excellent, and we rescheduled for a follow-up session in 7 days.
Two days after the second session, I got a text from Jen telling me that her neck was feeling awesome but, she was experiencing some low-back and thoracic symptoms of tightness and discomfort which began immediately after leaving my office. To me, this sounded a bit like the possibility of an ascending syndrome that might actually be originating from the hips and eventually ending up in her neck…maybe all a part of the overall layer syndrome posture.
A week later, Jen came in for her 3rd session. I explained what I thought the back symptoms might be coming from (the lower-cross syndrome/ascending syndrome idea). Then I tried to put it all together.
Jen indicated that her back discomfort seemed to be centered more on the right side at about the T12-L1 level. Her standing posture revealed a slightly lower right shoulder, and higher right hip. Her right lateral line was clearly compressed. I put her in a prone position on the table and tractioned her hips from the ankles. Upon releasing her ankles her right hip rebounded to a superior position compared to the left hip. I followed that with a check of her iliac crests and PSIS landmarks. Her right hip seemed a bit upslipped, so I palpated her QLs for tender points and found that her R QL was significantly facilitated and tender, compared to the left.
I began the treatment by releasing the R QL, returning it to its normal resting length (including stretching during therapy) and then moved inferiorly to the gluteus maximus, TFL, and ITB/hip abductors, repeating the process (I did not release the entire lateral line). The pelvic stabilization work balanced her hips and sacrum effectively and her back discomfort disappeared. Next, I worked through the shoulder and cervical protocols, just as I had done during Jen’s second visit.
To complete the session, we reviewed her home stretching/strengthening and I reiterated the importance of this aspect. Jen reports that she has been pain-free for the past month.
