Diagnosis
- Position: ESrightRleft
- Motion Restriction: Forward-bending, left side-bending, right rotation.
Treatment
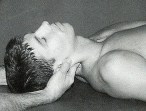
Patient is supine on the table with the operator sitting or standing at the head.
Operator’s left hand controls the patient’s occiput with the web of the thumb and the index finger along the soft tissues of the suboccipital area.
The operator’s right hand cups the chin with the index finger in front and the middle finger below the tip of the ramus. The operator’s right forearm is  placed along the right side of the patient’s head.
placed along the right side of the patient’s head.
Forward-bending is introduced by rotating the head forward by the operator’s hands around a transverse axis through the external auditory meatus.
Left side-bending and right rotation are introduced by the operator’s right forearm with slight left-to-right translation of the patient’s head to engage the restrictive barrier.  (Right rotation is not actively introduced)
(Right rotation is not actively introduced)
Patient instruction is to push the head directly posterior toward the table and into the hand offering resistance for 3-5 seconds of a mild isometric contraction. (An eye motion activating force is to look up toward the operator or toward the eyebrows.)
After relaxation, the operator engages the new forward-bending, left side-bending, and right rotational barriers.
Patient repeats the isometric contractions 3-5 times.
Retest.

 contact with the right side of the patients head.
contact with the right side of the patients head.


 Operator’s right hand is placed on the patient’s right frontoparietal region to control head movement.
Operator’s right hand is placed on the patient’s right frontoparietal region to control head movement.
 the flexion, right side-bending, and right-rotation restriction.
the flexion, right side-bending, and right-rotation restriction.








 monitoring the first movement of the atlas.
monitoring the first movement of the atlas.



 through the external auditory meatus while monitoring for the first movement of the atlas.
through the external auditory meatus while monitoring for the first movement of the atlas. to forward bending, right side-bending, and left rotation (ESleftRright). Something interfered with the left condyle’s ability to glide posteriorly.
to forward bending, right side-bending, and left rotation (ESleftRright). Something interfered with the left condyle’s ability to glide posteriorly. motion restriction is to forward bending, left side-bending, and right rotation (ESrightRleft). Something interfered with the right condyle’s ability to glide posteriorly.
motion restriction is to forward bending, left side-bending, and right rotation (ESrightRleft). Something interfered with the right condyle’s ability to glide posteriorly. restriction of the typical cervical segment rotation through ligamentous locking. Neck flexion must be maintained throughout the procedure.
restriction of the typical cervical segment rotation through ligamentous locking. Neck flexion must be maintained throughout the procedure. rotated left).
rotated left). rotated right).
rotated right).
 his index fingers. If resistance is felt, the motion restriction is to forward-bending, right side-bending, and right rotation (indicating that the segment is extended, rotated and side-bent left [ERSleft]). Something has interfered with the capacity of the left facet to open.
his index fingers. If resistance is felt, the motion restriction is to forward-bending, right side-bending, and right rotation (indicating that the segment is extended, rotated and side-bent left [ERSleft]). Something has interfered with the capacity of the left facet to open. his index fingers. If resistance is felt, the motion restriction is to forward-bending, left side-bending, and left rotation (indicating that the segment is extended, rotated, and side-bent right [ERSright]). Something has interfered with the capacity of the right facet to open.
his index fingers. If resistance is felt, the motion restriction is to forward-bending, left side-bending, and left rotation (indicating that the segment is extended, rotated, and side-bent right [ERSright]). Something has interfered with the capacity of the right facet to open.


 operator introduces translation from right to left, sensing for resistance to movement at his index fingers. If resistance is felt, the motion restriction is to backward-bending, right side-bending, and right rotation (indicating that the segment is flexed, rotated and side-bent left [FRSleft]). Something has interfered with the capacity of the left facet to close.
operator introduces translation from right to left, sensing for resistance to movement at his index fingers. If resistance is felt, the motion restriction is to backward-bending, right side-bending, and right rotation (indicating that the segment is flexed, rotated and side-bent left [FRSleft]). Something has interfered with the capacity of the left facet to close. operator introduces translation from left to right, sensing for resistance to movement at his index fingers. If resistance is felt, the motion restriction is to backward-bending, left side-bending, and left rotation (indicating that the segment is flexed, rotated, and side-bent right [FRSright]). Something has interfered with the capacity of the right facet to close.
operator introduces translation from left to right, sensing for resistance to movement at his index fingers. If resistance is felt, the motion restriction is to backward-bending, left side-bending, and left rotation (indicating that the segment is flexed, rotated, and side-bent right [FRSright]). Something has interfered with the capacity of the right facet to close.



