A. In the absence of dysfunction, side-bending of the typical cervical spine to the right allows the right facet to close and the left facet to open. Side-bending to the left allows the left facet to close and the right facet to open.
In determining if a facet can close, one would bias the paired facets into extension by translating the vertebral segment anteriorly. From there, translating that segment from right to left tests the right side’s ability to close, while translating from left to right tests the left side’s ability to close.
In determining if a facet can open, one would bias the paired facets into flexion by translating the vertebral segment posteriorly. From there, translating that segment from right to left tests the left side’s ability to open, while translating that segment from left to right tests the right side’s ability to open.
B. In the absence of dysfunction, side-bending the occiput to the right (right to left translation) onto the superior articular facet of C1 causes the right condyle to glide anteriorly (extend) on C1 and the left condyle to glide posteriorly (flex) on C1.
In determining if the condyles can symmetrically glide anterior or extend, one would bias the occiput into extension by translating the condyles anteriorly on the superior articular facets of C1 (backward bending). From there, side-bending the occiput to the right further tests the right side’s ability to extend. Side-bending the occiput to the left (left to right translation) further test the left side’s ability to extend.
In determining if the condyles can symmetrically glide posterior or flex, one would bias the occiput into flexion by translating the condyles posteriorly on the superior articular facets of C1 (forward bending). From there, side-bending the occiput to the right further tests the left side’s ability to flex; side-bending to the left further tests the right side’s ability to flex.
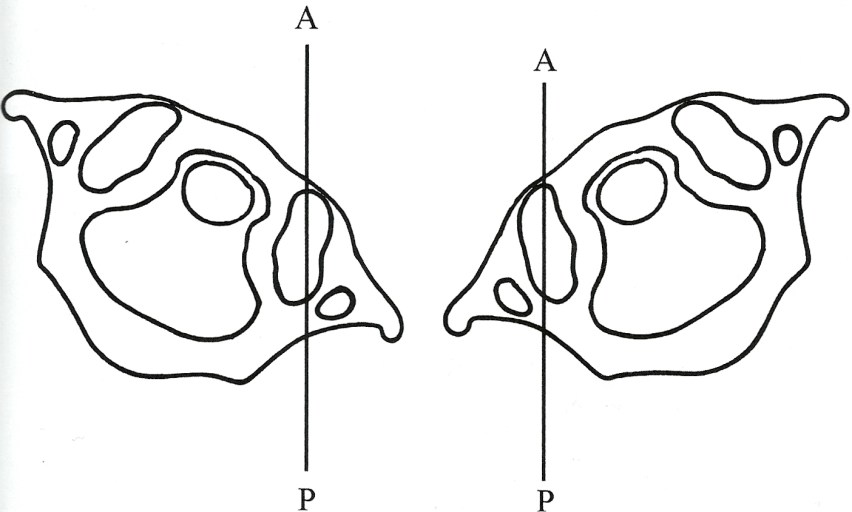
C. The articular structures of C0-C1 are unique. Relative to the anterior/posterior (sagittal plane), the anterior aspect of the articulating surface sits 30˚ medial to the posterior aspect of the articular surface. Turning the occiput and C1 (atlas) to the right 30˚ places the right C0-C1 articular surface parallel to the A/P (anterior/posterior) plane. Turning the occiput and C1 to the left 30˚ places the left articular surface parallel to the A/P plane.



 resistance to movement at his index fingers. If resistance is felt, motion restriction is to backward bending, right side-bending, and left rotation (C0 flexed [F], side-bent left [Sleft], and rotated [Rright]. Something interfered with the right condyle gliding forward.
resistance to movement at his index fingers. If resistance is felt, motion restriction is to backward bending, right side-bending, and left rotation (C0 flexed [F], side-bent left [Sleft], and rotated [Rright]. Something interfered with the right condyle gliding forward. encountered, the restriction is to backward bending, left side-bending, and right rotation (FSrightRleft). Something interfered with the left condyle gliding forward.
encountered, the restriction is to backward bending, left side-bending, and right rotation (FSrightRleft). Something interfered with the left condyle gliding forward. rotation of the head sensing for prominent fullness under the right thumb indicating posterior rotation of the atlas on the left.
rotation of the head sensing for prominent fullness under the right thumb indicating posterior rotation of the atlas on the left. and left rotation of the head and monitors for prominence of the right posterior arch of the atlas under the right index finger, indicative of right rotation of the atlas.
and left rotation of the head and monitors for prominence of the right posterior arch of the atlas under the right index finger, indicative of right rotation of the atlas. rotation with the left hand while monitoring for prominence of the right posterior arch of the atlas under the right index finger, indicating atlas right rotation.
rotation with the left hand while monitoring for prominence of the right posterior arch of the atlas under the right index finger, indicating atlas right rotation. rotation of the head with the left hand while monitoring for prominence of the left posterior arch of the atlas under the right thumb, indicating left rotation of the atlas.
rotation of the head with the left hand while monitoring for prominence of the left posterior arch of the atlas under the right thumb, indicating left rotation of the atlas.





 thumb.
thumb.



