Gait Pattern Mat Routine from TheCastleMethod
The Gait Pattern (Walking Cycle)
(If this article is too technical for your interest, cut to the chase and just read the ***three-starred portions. I’m suggesting that dysfunctional gait patterns can be the cause (source) of low-back pain, functional evaluation of gait can diagnose the cause of pain, and functional gait pattern training can be utilized to correct the problem.)
Current healthcare statistics have revealed that 80% ( the vast majority) of us are going to experience some type of back pain during our lives. That’s quite a lot of people. These statistics also indicate that 60-80% of (low) back pain cases are classified as ‘idiopathic’.
Definition: [Idiopathic], relating to or denoting any disease or condition that arises spontaneously or for which the cause is unknown.
***The cause of idiopathic (low) back pain can often be found in a dysfunctional gait pattern. Because idiopathic (low) back pain is not a ‘structural lesion’, it can’t be diagnosed through imaging (MRI). It is a ‘functional lesion’ which can only be diagnosed through functional assessment.
Lisa DeStefano, DO, in Greenman’s Principles of Manual Medicine, (2011), discusses this issue:
*** “The differential diagnosis of low back pain continues to be a dilemma for the examining physician. Approximately 60-80% of cases of low back pain are still classified as idiopathic. After the exclusion of structural lesions and organic pathologies by orthodox orthopedic and neurological testing, the examiner is left with the difficulty of determining if any other treatable source for the back pain can be identified. It is in these patients that the ability to identify and treat functional abnormalities of the musculoskeletal system has been found to be clinically effective. Including functional diagnosis of these patients significantly reduces the numbers that need to be classified as idiopathic.”
Traditional gait analysis assumes that “healthy people”- have a “normal” gait. For instance, gait analysts will often explain what “the” gluteus maximus muscle is doing – as if there was only one way of walking. This type of analysis contradicts the common observation that there are many different gaits. However, even among people regarded as clinically healthy, ***there are great variations of gait style, some of which can, and will promote the development of (low) back pain.
***The manner in which our axial complex alternately undulates in side-bending and rotation as we walk is necessary to the maintenance of pain-free movement. This highly complex movement pattern is the result of the integration of many smaller movement patterns that all come together in a functional gait pattern.
Regardless of individual gait style variations, there are certain kinematics that must be adhered to in order to perform the gait pattern in a pain-free manner.
Side-bending and rotation of the sacrum are also called ‘torsion’. Proper body movement while walking is influenced by the ability of the sacrum to torsion left on the left axis and right on the right axis.
Sacral torsional movement is considered to occur around an oblique axis. By convention, the left oblique axis runs from the upper extremity of the left sacroiliac joint to the lower end of the right sacroiliac joint, and the right oblique axis runs from the upper end of the right sacroiliac joint to the lower extremity of the left sacroiliac joint.
Clinical observation of the normal walking cycle demonstrates that sacral side-bending and rotation couple to opposite sides. This is also known as ‘Type 1 motion’.
‘Type 2 motion’ designates coupling to the same side (i.e. rotating right and side-bending right).
The anterior and posterior movement of the sacral base is called nutation and counter-nutation, respectively. The simpler designations of anterior nutation and posterior nutation are often used when referring to this motion. The word ‘nutation’ means ‘nodding’.
With left torsion on the left oblique axis, the sacrum rotates left and side-bends right, with the right sacral base moving into anterior nutation.
With right torsion on the right oblique axis, the sacrum rotates right and side-bends left, with the left sacral base moving into anterior nutation.
Because the nutational component of this normal walking movement is anterior in direction, left torsion on the left oblique axis (L on L) and right torsion on the right oblique axis (R on R) are described as anterior torsional movements.
Although the exact biomechanics of the torsional movements of the sacrum are unknown, the hypothetical left and right oblique axes are useful for descriptive purposes. The nutational movement in normal walking is anterior on one side, return to neutral, and anterior to the opposite side, and return to neutral.
***Because much of the activity of the musculoskeletal system involves the walking cycle, maintenance of normal L-on-L and R-on-R sacral torsion is critical for pain-free movement. With (lower) back pain, functional gait kinematics should be a therapeutic objective of the highest priority.
At right heel strike, the right innominate has rotated in a posterior direction and the left innominate has rotated in an anterior direction. The anterior surface of the sacrum is rotated to the left and the superior surface is level.
As your right leg moves from heel strike to toe-off, your body weight begins to move over your right leg, causing your pelvis to shift laterally to the right. At right leg mid-stance, the right leg is straight and the innominate is rotating anteriorly. The sacrum has rotated right and side-bent left.
As the movement continues toward right leg toe off, your right pelvic innominate bone begins to rotate anteriorly while your left innominate bone begins to rotate posteriorly.
As your right innominate rotates anteriorly, your sacrum moves into right torsion on the right oblique axis (i.e., right rotates and left side-bends because the left sacral base moves in anterior nutation).
Your lumbar spine side-bends right and rotates left, your thoracic spine side-bends left and rotates right and your cervical spine side-bends right and rotates right.
At left heel strike, the left innominate begins to rotate anteriorly; after toe-off, the right innominate begins to rotate posteriorly. The sacrum is level, rotated right.
At left leg mid-stance, the left innominate is high, rotating anteriorly, and the left leg is straight. The sacrum has rotated to the left and is side-bent right.
As your left innominate rotates anteriorly, your sacrum moves into left torsion on the left oblique axis (i.e., left rotates and right side-bends because the right sacral base moves in anterior nutation).
As your left leg moves from weight bearing to toe off, the left innominate, the sacrum, lumbars and thoracics torsion, rotate and side-bend in an opposite manner.
Notice how this same complex pattern of pelvic shift, sacral torsion, side-bending, and rotation is introduced as the weight of the body is shifts to rest on the left leg. ***Walking and standing with your weight over one leg introduces and requires this particular curvature for normal, pain-free movement.
AACOM (American Association of Colleges of Osteopathic Medicine) Videos
Sacral Motion Through the Gait Cycle
Purpose: Normal gait cycle mechanics of the sacrum, innominates and lumbar spine. Normal physiologic motion of both left on left and right on right at different phases of the gait cycle is illustrated. When there is a restriction, it becomes a somatic dysfunction, specifically a forward sacral torsion, either left on left or right on right.
Right-on-Right Torsion
Purpose: Starting with an expansion of the innominates and the sacrum, the motion of a right on right sacral torsion is demonstrated. Also note the relative movements of the ilia and, to a lesser degree, the lumbar vertebra. This is normal sacral motion as part of the gait cycle.
Posterior Innominate Motion with Related Sacral Motion
Purpose: Intended to build upon the relationship of innominate diagnosis, in this case an inferior PSIS and anterior ASIS, with the motion of the sacrum, a physiologic left on left motion which, if restricted would become a somatic dysfunction, a left on left sacral torsion which may be the cause of or the result of the posterior innominate also being restricted.
Right Anterior Innominate Motion
Purpose: Illustrates the relationship between normal innominate motion, in this case anterior rotation, and the corresponding motion of the sacrum, rotation about a right axis.
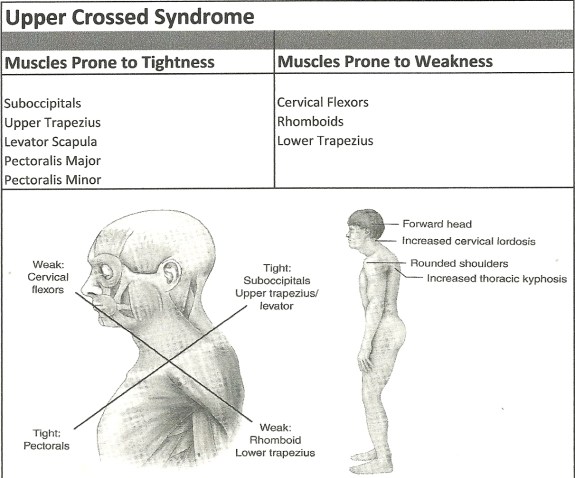
 The function of the intrinsic cervical flexors is to produce forward sagittal plan rotation or ‘rolling’ of the cervical vertebrae. The muscles producing the sagittal rotation motion in the upper cervical region are the rectus capitis anterior and rectus capitis lateralis.
The function of the intrinsic cervical flexors is to produce forward sagittal plan rotation or ‘rolling’ of the cervical vertebrae. The muscles producing the sagittal rotation motion in the upper cervical region are the rectus capitis anterior and rectus capitis lateralis.






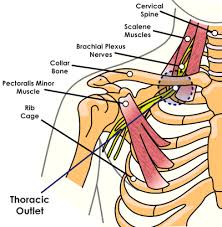
 Impingement is caused by narrowing of the SAS (subacromial space) either due to boney growth (primary impingement) or superior migration of the humeral head caused by weakness or muscle imbalance (secondary impingement). The result is inflammation or damage to the rotator cuff tendons; therefore, chronic impingement can lead to rotator cuff tendinosis. As secondary impingement is related to glenohumeral instability, it is sometimes described as functional instability; it occurs mostly in athletes less than 35 years of age who use overhead throwing motions.
Impingement is caused by narrowing of the SAS (subacromial space) either due to boney growth (primary impingement) or superior migration of the humeral head caused by weakness or muscle imbalance (secondary impingement). The result is inflammation or damage to the rotator cuff tendons; therefore, chronic impingement can lead to rotator cuff tendinosis. As secondary impingement is related to glenohumeral instability, it is sometimes described as functional instability; it occurs mostly in athletes less than 35 years of age who use overhead throwing motions.