Excerpted from: (Page, Frank, Lardner. Assessment and Treatment of Muscle Imbalance, The Janda Approach. 2010, Human Kinetics, Champagne IL.)
Muscle tension (tone) is the force with which a muscle resists being lengthened. Muscle tension may also relate to a muscle’s activation potential or excitability; thus, testing muscle tension has two components: viscoelastic and contractile. The viscoelastic component relates to the extensibility of structures, while the contractile component relates to the neurological input.
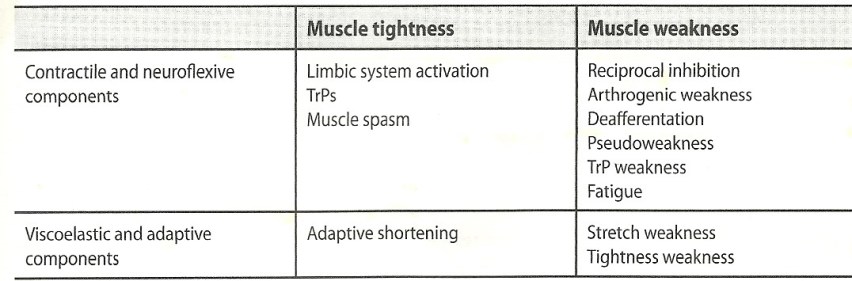
Contractile and Non-contractile Components of Muscle Tightness and Weakness
Muscle Tightness
Muscle tightness is the key factor in muscle imbalance. Muscles prone to tightness are typically one third stronger than muscles prone to inhibition. Muscle tightness creates a cascade of events that lead to injury. Tightness of a muscle reflexively inhibits its antagonist, creating muscle imbalance. This muscle imbalance leads to joint dysfunction because of the unbalanced forces. Joint dysfunction creates poor movement patterns and compensations, leading to early fatigue. Overstress of activated muscles and poor stabilization lead to injury.
There are three important factors in muscle tightness: muscle length, irritability threshold, and altered recruitment. Muscles that are tight are usually shorter than normal and display an altered length-tension relationship. Muscle tightness leads to a lowered activation threshold or lowered activation threshold, which means that the muscle is readily activated with movement. Movement typically takes the path of least resistance, and so tight and facilitated muscles are the first to be recruited in movement patterns. Tight muscles typically retain their strength, but in extreme cases they can weaken.
Structurally, increased muscle tension is caused by a lesion of the CNS that results in spasticity or rigidity. Tight muscles are also described as hypertonic or facilitated. Functionally, increased muscle tension results from either neuroflexive or adaptive conditions. These two conditions are based on the contractile (neuroflexive factors) and viscoelastic (adaptive factors) components of muscle tension.
Neuroflexive Factors for Increased Tension
Limbic System Activation
Stress, fatigue, pain, and emotion contribute to muscle tightness through the limbic system. Muscle spasms due to limbic system activation usually are not painful but are tender to palpation. They are most frequently seen in the shoulders, neck, and low back and in tension headache.
Trigger Points (TrPs)
TrPs are focal areas of hypertonicity that are not painful during movement but are painful with palpation. Essentially, they are localized, hyperirritable taut bands within muscle.
Muscle Spasm
Muscle spasm causes ischemia or an altered movement or joint position resulting from altered tension. The spasm itself does not cause pain because spasm is not associated with increased EMG activity. Muscle spasm is a typical response to joint dysfunction or pain irritation due to an impairment of interneuronal function at the spinal level. Muscle spasm leads to a reflex arc of reciprocal inhibition for protection and subsequently impaired function of the motor system. These muscles are also tender to palpation.
Adaptive Factors for Increased Tension
Increased muscle tension also results from adaptive shortening. Over time, muscle remains in a shortened position, causing a moderate decrease in muscle length and subsequent postural adaptation. Adaptive shortening is often considered overuse. These muscles are not painful at rest but are tender to touch. They exhibit a lowered irritability threshold and are readily activated with movement. Over the long term, strength decreases as active fibers are replaced by non-contractile tissue. It is thus extremely important for the clinician to identify the cause of increased muscle tension in order to apply the appropriate treatment.
Causes of Muscle Weakness
Muscle tension can decrease as a result of a structural lesion in the CNS such as a spinal cord injury or stroke. A loss of tension leads to flaccidity or weakness. Weak muscles are also describes as hypotonic or inhibited. Functionally, muscle can be weak as a result of neuroflexive or adaptive changes and may exhibit delayed activation in movement patterns.
Neuroflexive Factors for Decreased Tension
Many contractile factors can contribute to decreased muscle tension.
Reciprocal Inhibition: Muscle becomes inhibited reflexively when its antagonist is activated. Weakness is often reflex-mediated inhibition secondary to increased tension of the antagonist.
Arthrogenic Weakness: Muscle becomes inhibited via anterior horn cells due to joint swelling or dysfunction. This weakness also leads to selective atrophy of Type II fibers.
Deafferentation: Deafferentation is a decrease in afferent information from neuromuscular receptors. Damage to joint mechanoreceptors (as seen with ligamentous injury) with subsequent loss of articular reflexes can cause altered motor programs, often influencing many muscles remote from the injured area. This loss of afferent information ultimately leads to de-efferentation, or the loss of efferent signals to alpha motor neurons, which results in decreased muscle strength.
Pseudoperesis: Pseudoperesis is a clinical presentation of neuroflexive origin. Pseudoperesis has three clinical signs: Hypotonia upon inspection and palpation, a score of 4/5 on a manual muscle test,and a change in the muscle activation pattern that may include delayed onset with early synergist activation or decreased EMG levels. Faciliatory techniques often restore muscle strength and activation, but can also be inhibitory to a pseudoparetic muscle.
TrP Weakness: Hyperirritable bands of muscle fiber decrease the stimulation threshold, leading to overuse, early fatigue, and ultimately weakness. Muscles with active TrPs fatigue more rapidly than normal muscles and they exhibit a decreased number of firing motor units and poor synchronization.
Fatigue: Muscle fatigue can be cause by metabolic or neurological factors. Often during exercise muscles are fatigued before pain is experienced. Thus the patient develops compensatory and faulty movement patterns before experiencing pain.
Adaptive Factors for Decreased Tension
Non-contractile factors causing decreased muscle tension are:
Stretch Weakness: Stretch weakness is a condition in which muscle is elongated beyond physiological neutral but not beyond normal ROM. Prolonged muscle elongation causes muscle spindle inhibition and the creation of additional sarcomeres. The increased muscle length also changes the length-tension curve. Stretch weakness is also known as positional weakness and is often associated with overuse and postural changes. There is also an increase in the non-contractile tissue and a decrease in elasticity, leading to hypertrophy. Ultimately overuse leads to ischemia and degeneration of muscle fibers, which further weakens the muscle.
When an inhibited and weak muscle is resisted, as is the aim of strengthening exercises, its activity tends to decrease rather than increase. It is important to distinguish between neuroflexive weakness and structural weakness. Often if the tight antagonist is stretched, the weak and inhibited muscle spontaneously increases in strength.





