Excerpted from Page, Frank, and Lardner. Assessment and Treatment of Muscle Imbalance: The Janda Approach (2010)
Neurological chains are seen in the sensorimotor system and in neurodevelopmental movement patterns.
The sensorimotor system is linked neurologically through the afferent and efferent systems. In controlling movement, feedback and feed forward mechanisms provide a chain reaction of neuromuscular events. This provides both global and local stabilization of joints through muscular chains. These sensorimotor chains are affected by afferent input, controlled by the CNS, and realized through efferent motor output.
Simply put, groups of muscles are linked together neurologically for function…
Sensorimotor chains include reflex stabilization chains and adaptation chains.
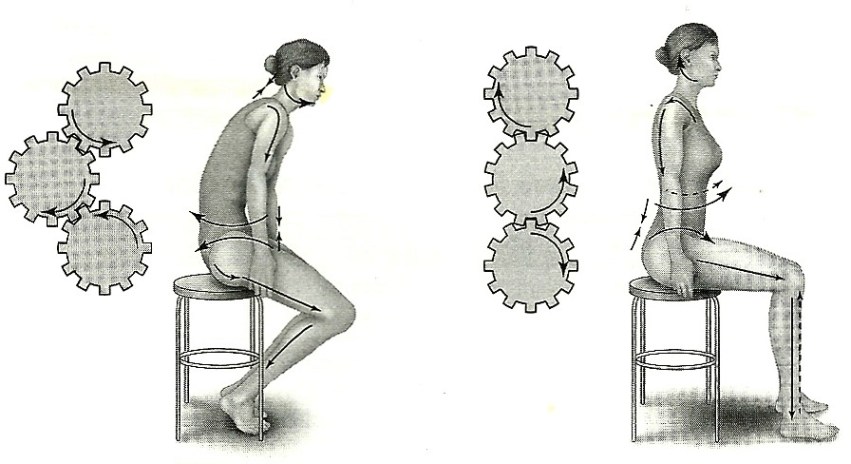
Reflex stabilization is an example of a functional neurological chain reaction. Reflex stabilization occurs subconsciously. Muscles contract involuntarily to provide stabilization either locally or globally. As an example, in the standing posture if an anterior weight shift occurs, the posterior dorsal muscles are activated, while a posterior weight shift activates the anterior ventral muscles.
Sensorimotor influence for spinal muscle stabilization is demonstrated by activation of the contralateral erector spinae during ipsilateral shoulder abduction.
The most important stabilizing sensorimotor chain is the pelvic chain, consisting of the TrA, multifidus, diaphragm, and pelvic floor. These four muscles are coactivated for trunk stability and force transmission. The pelvic chain is the cornerstone of stability for the rest of the body. This is probably why Waslaski suggests that a pelvic stabilization sequence should be performed as the prelude to all other protocols in a pain model session.
Pelvic weakness has been associated with low back pain, groin strains, IT band syndrome, anterior knee pain, ACL tears, and ankle sprains. Janda was one of the first to note delayed firing of the TrA in patients with chronic low back pain. Patients with functional ankle instability change their postural stabilization by introducing a hip strategy, while subjects without instability favor an ankle strategy.
Similar pathologies are noted in the shoulder by delayed activation of the mid- and lower trapezius as well as the serratus anterior (scapular stabilization) in swimmers with shoulder impingement.
Janda identified two types of sensorimotor adaptation chains: horizontal (anatomic) adaptation and vertical (neurological) adaptation.
Horizontal adaptation occurs when impaired function in one joint or muscle creates a reaction and adaptation in other joint segments. It is most commonly seen in the spine, where low back pain often leads to cervical syndromes. Muscle imbalances conform to horizontal adaptation and actually create predictable patterns that can be observed as proximal to distal or distal to proximal. The distal to proximal pattern is seen most often in the case of ankle sprains, where researchers have found weakness and other changes in hip muscle(s) activation.
Vertical adaptation occurs between the PNS and CNS, where adaptation in one part of the sensorimotor system impairs the function of the entire system. The adaptation can progress from the PNS to the CNS, or CNS to PNS, and can be observed as a change in the motor programming that results in abnormal movement patterns. A good example would be where an individual with functional ankle instability exhibits altered kinematics during gait. This type of compensation is known as a ‘feed forward’ change in the motor control program.
Neurological Locomotor Patterns
Two groups of muscles are regulated throughout the body by the CNS; the tonic muscle system and the phasic muscle system. There are several ways to differentiate between these two groups. Neurologically, tonic and phasic refer to their classification in neurodevelopmental movement patterns.
Tonic system muscles are older phylogenetically and are dominant. They are involved in repetitive or rhythmic activities. Their function is predominantly that of flexion.
Phasic system muscles are more predominant in extension movements. They are younger phylogenetically and typically work against gravity, acting as postural stabilizers.
The tonic and phasic systems do not function individually. They work together through coactivation for posture, gait, and coordinated movement. Janda’s concept of muscle balance is based on an interaction of the tonic and phasic systems for optimal posture and movement. This interaction provides for centration of joints during movement, creating a balance of muscular forces that maintain joint congruency through movement. This is somewhat different than other concepts of muscle balance that are described only in terms of length/strength relationships.
When these two systems are coactivated in specific chains of movement, each chain is made up of a series of synergistic movements that are combined into coordinated movement patterns. These movement patterns serve as the default motor program on which humans base more complicated movements. Upper-quarter (cervical and upper-extremity) tonic-phasic coactivation patterns are used for prehension, grasping, and reaching. Lower-quarter (lumbar and lower-extremity) patterns are used for creeping, crawling, and gait.
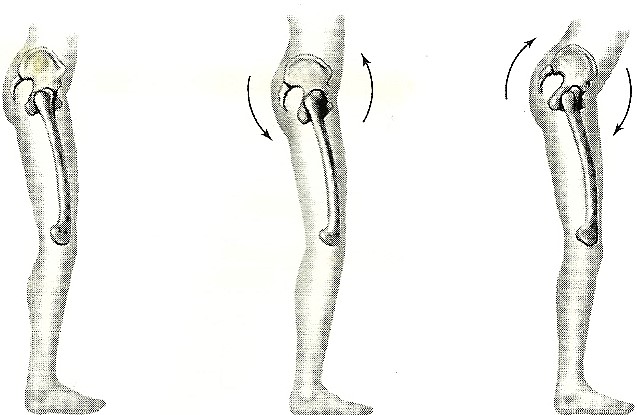
Proper balance of these two systems is demonstrated in normal gait and posture. The integration of the tonic and phasic systems between the lower and upper body is responsible for reciprocal locomotion. Specifically, the coactivation of the contralateral upper- and lower-quarter systems throughout the body produces the characteristic patterns of reciprocal arm and leg movements. During the swing phase, the left lower-extremity performs a tonic movement pattern (hip flexion). At the same time the right upper-extremity performs a tonic pattern (shoulder flexion). While the right lower-extremity performs the stance phase (hip extension) a phasic movement pattern, the left upper-extremity performs the phasic movement pattern of shoulder extension. This demonstrates the reciprocal coactivation of the tonic and phasic systems in a movement pattern known as gait (walking).

Understanding chain reactions helps practitioners quickly identify and predict functional pathology. The concept of chain reactions emphasizes the clinical principle of looking beyond the site of the pain to focus on the cause rather than the source of pain.




 Understanding the function and pathsof these slings is necessary for clinicians to correctly diagnose and treat challenging musculoskeletal pain syndromes. For example right shoulder pain may be related to left hip dysfunction, and vice versa…and may present clinically as pain, muscle imbalances, or trigger points within the sling.
Understanding the function and pathsof these slings is necessary for clinicians to correctly diagnose and treat challenging musculoskeletal pain syndromes. For example right shoulder pain may be related to left hip dysfunction, and vice versa…and may present clinically as pain, muscle imbalances, or trigger points within the sling.