Frozen shoulder is the term commonly used to refer to ‘adhesive capsulitis’. True frozen shoulder includes a variety of pathologies that may include adhesive capsulitis, subacromial bursitis, tendinosis, rotator cuff injuries, and other clinical conditions limiting shoulder motion. Adhesive capsulitis involves loss of active and passive motion due to adhesions within the glenohumeral joint capsule.
An accident, trauma, emotional or physical stress, repetitive movements, or overuse (too much too soon) can lead to immobilization or lack of full range of motion of the shoulder. When this occurs, adhesions can build up in the shoulder joint capsule and cause adhesive capsulitis. A client with this condition may have a combination of limited flexion, abduction, or external rotation. The greatest restriction is typically abduction and external rotation.
Early on adhesive capsule involvement initially causes a bone-on-bone-like end feel in lateral rotation, followed closely by the same end feel in abduction usually limiting abduction to 35-45˚. The end feel on a passive range of motion test will appear to be bone-on-bone-like. Simple conditions such as supraspinatus impingement and bursitis could lead to frozen shoulder due to prolonged immobility and limited shoulder movement.
Dr. Erik Dalton has commented that the shoulder joint capsule has a considerable amount of slack, loose tissue so the shoulder is unrestricted through its large range of motion. However in clients with a true adhesive capsulitis, inflammation in the joint makes the normally loose (inferior) parts of the joint capsule stick together. In his opinion, this is usually caused by a fibrin deposition from dried inflammatory waste products. As gravity slowly pulls the waste products into the lower (plicated) capsular folds, the area becomes dehydrated and causes fibrin deposition to glue down the capsule. The more inflammation, the more fibrosis, thus the capsule slowly fills up until the entire capsule is infiltrated. This seriously limits the shoulder’s ability to move and causes the shoulder to freeze. Dalton believes that most frozen shoulders are caused by supraspinatus tendinitis, autoimmune problems, and lack of daily stretching.

Remember, causes of frozen shoulder can be secondary to supraspinatus impingement, rotator cuff tears, labrum tears, emotional contributions, prolonged shoulder immobilization, and postsurgical complications.
Treatment:
- Pain-free joint capsule work is imperative for success in treating this condition. (see Joint Capsule Work in (Waslaski, Clinical Massage Therapy: A Structural Approach to Pain Management, Pearson Education Inc., 2012, page 156).
This unique technique is one of Waslaski’s trademark techniques. It should be utilized whenever any shoulder range of motion end feel appears to be bone-on-bone-like. Caution! This technique should be learned only under the instruction and direct supervision of James Waslaski. Please do not attempt to utilize this technique without special training, because you can easily injure your client if the technique is used incorrectly, or inappropriately. The following is merely a brief introduction to this technique.
With the client supine, abduct the arm to the first bone-on-bone-like restriction
- With one hand, using evenly displaced pressure, support and stabilize the scapula from either on top of or under the client’s shoulder, so that it does not move.
- Use your other hand to hold the arm just proximal to the elbow.
- Perform a gentle plunging technique using the head of the humerus as a massage tool. This mimics a mortar and pestle effect. Gently and slowly compress the humerus into the joint capsule simulating your hands coming together.
- Check the discomfort level with the client. There usually isn’t any discomfort though, as you are actually shortening the fascial adhesions and taking pressure off the joint capsule. Encourage the client to relax and visualize the capsule softening and letting go.
- Make contact in the joint capsule, using the cartilage of the humerus to massage the fascia that is gluing it against the fascia of theof the scapula (glenoid).
- Rotate the arm gently, and then pull back out. Contact the scapula, rotate the humerus, and then decompress the scapula. Continually repeating this sequence allows the head of the humerus to soften and mobilize the fascia deep within the joint capsule. What creates myofascial release is heat, pressure, movement, and slow-velocity fascial stretching.
- Make your plunges nonsynchronized and then slowly stretch the inner fascia and surrounding joint capsule.
- Rotate the arm externally to the restriction and repeat the plunging technique several times. Then perform a deep fascial and capsular stretch externally. Back off the stretch, return to neutral position, and then pull back out of the joint capsule.
Compression Decompression


Internal Rotation External Rotation


You must rotate the arm to the left and right because there could be multiple adhesions in different directions and at different degrees of abduction. Most people have more lateral rotation restriction due to tight medial shoulder rotators, therefore more restrictions will usually be found as you move toward lateral rotation and move further into abduction.
You may feel (hear) some popping and releasing of the fascia as you create more freedom in the joint capsule. It is critical to perform this work totally pain-free, as even minor guarding prevents effective joint capsule work.
- Start with this and progress through the shoulder protocol (see ) returning to the joint capsule work when necessary. At any point when you are balancing out the muscle groups of the shoulder, if there is a bone-on-bone-like end feel, perform this revolutionary capsule work.
- Continue to reassess the client’s range of motion and end feel until it is pain free.
- Have the client discontinue any strengthening exercises except those for rhomboids, lower trapezius, infraspinatus, and teres minor, that help stabilize excessive upward scapular movement.
- Give the client homework in the form of stretches specific to the restricted muscles and pain-free range of motion for neuromuscular reeducation.
If the fascial adhesions inside of the joint capsule are released, and the fibrosis of the capsule itself is immobilized, the client must take the shoulder through each full range of motion daily to prevent adhesions from forming again. The worst thing to do in clients with adhesive capsulitis is immobilize their shoulder.
 The subacromial bursa is located underneath the acromiom, to prevent compression of soft tissue against the bone. This fluid-filled sac has two major sections and most of it is inaccessible. The more distal portion is the subdeltoid bursa. When the arm is fully abducted, the bursa moves up under the acromiom process. The bursa can be agitated by repetitive compression of the humerus into the acromiom due to a tight upper trapezius, middle deltoid, and supraspinatus muscle. An indicator of bursitis is when shoulder pain begins shortly after initiating shoulder abduction, and continues to about 135˚. This is called a painful arc, which happens because the irritated bursa is compressed as the client abducts the shoulder. After 135˚ of abduction, the irritated tissue moves proximally under the acromiom process and is no longer compressed. The pain is described as being deep within the shoulder joint.
The subacromial bursa is located underneath the acromiom, to prevent compression of soft tissue against the bone. This fluid-filled sac has two major sections and most of it is inaccessible. The more distal portion is the subdeltoid bursa. When the arm is fully abducted, the bursa moves up under the acromiom process. The bursa can be agitated by repetitive compression of the humerus into the acromiom due to a tight upper trapezius, middle deltoid, and supraspinatus muscle. An indicator of bursitis is when shoulder pain begins shortly after initiating shoulder abduction, and continues to about 135˚. This is called a painful arc, which happens because the irritated bursa is compressed as the client abducts the shoulder. After 135˚ of abduction, the irritated tissue moves proximally under the acromiom process and is no longer compressed. The pain is described as being deep within the shoulder joint. This is a common condition seen in both athletes and non-athletes as these muscles tend to be weak, overstretched, and prone to injury. It is a common early season condition seen in baseball players, especially pitchers. Throwing a ball at 100 mph involves powerful muscles such as the pectoralis major, subscapularis, and deltoid.
This is a common condition seen in both athletes and non-athletes as these muscles tend to be weak, overstretched, and prone to injury. It is a common early season condition seen in baseball players, especially pitchers. Throwing a ball at 100 mph involves powerful muscles such as the pectoralis major, subscapularis, and deltoid.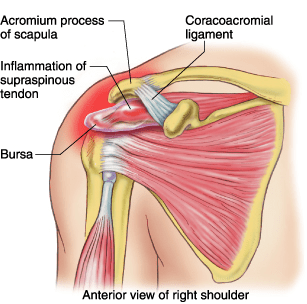 Supraspinatus tendonitis is a misleading term, because in many cases by the time the client presents to the therapist he or she no longer has inflammation. A better term would be tendon pain or tendinosis, which is the tearing of tendon fiber sin the absence of an inflammatory process.
Supraspinatus tendonitis is a misleading term, because in many cases by the time the client presents to the therapist he or she no longer has inflammation. A better term would be tendon pain or tendinosis, which is the tearing of tendon fiber sin the absence of an inflammatory process. Since the rotator cuff involves a group of four muscles, you must perform a thorough assessment to determine which of the muscles are involved: supraspinatus, infraspinatus, teres minor, or subscapularis. It is not uncommon for an athlete to be diagnosed with a rotator cuff injury and actually have bicipital tendinosis.
Since the rotator cuff involves a group of four muscles, you must perform a thorough assessment to determine which of the muscles are involved: supraspinatus, infraspinatus, teres minor, or subscapularis. It is not uncommon for an athlete to be diagnosed with a rotator cuff injury and actually have bicipital tendinosis. muscles are involved. The most common muscle to be injured is the supraspinatus , because it is often impinged due to a tight subscapularis, pectoralis minor, upper trapezius, and middle deltoid leading to strained fibers as it moves under the acromiom, as well as the teres minor because it is usually weak and inhibited and placed under extreme eccentric forces during deceleration of the shoulder, especially in athletes.
muscles are involved. The most common muscle to be injured is the supraspinatus , because it is often impinged due to a tight subscapularis, pectoralis minor, upper trapezius, and middle deltoid leading to strained fibers as it moves under the acromiom, as well as the teres minor because it is usually weak and inhibited and placed under extreme eccentric forces during deceleration of the shoulder, especially in athletes.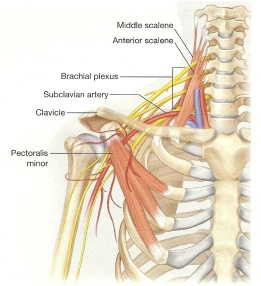 Thoracic Outlet can include several variations of nerve or vascular compression near the base of the neck and upper rib cage. Compression at the superior thoracic outlet is common and the most understood portion involves compression of the neurovascular bundle passing between the anterior and middle scalenes, also known as Anterior Scalene Syndrome. This part compresses the brachial plexus of nerves and brachial artery. Because the subclavian vein does not pass between the scalene muscles, there are usually only nerve compression symptoms present such as pain, tingling, and numbness in the arms and hands.
Thoracic Outlet can include several variations of nerve or vascular compression near the base of the neck and upper rib cage. Compression at the superior thoracic outlet is common and the most understood portion involves compression of the neurovascular bundle passing between the anterior and middle scalenes, also known as Anterior Scalene Syndrome. This part compresses the brachial plexus of nerves and brachial artery. Because the subclavian vein does not pass between the scalene muscles, there are usually only nerve compression symptoms present such as pain, tingling, and numbness in the arms and hands.